General
- Assess risk for hospital acquired VTE at time of admission, change in level of care, and discharge.
- Educate patients about signs and symptoms of VTE, as well as VTE prophylaxis.
- Ambulate patients early and frequently - set daily activity goals.
Medical (Non-Surgical) Patients
- ICU patients: Unless contraindicated, most patients should receive pharmacologic prophylaxis.
- Non-ICU patients: Several risk stratification models for hospital acquired VTE exist, including the Padua Score, the Improve Score, and the Geneva Score. Choose one to guide decision for VTE prophylaxis.
- Pauda score ≥ 4 → 11% risk VTE without prophylaxis; pharmacologic VTE prophylaxis recommended (some recommend cut off of ≥3).
- Improve score ≥ 3-4 → 7-11% risk of VTE; pharmacologic VTE prophylaxis recommended.
- Geneva Score ≥ 3 → ~3.5% risk of VTE; pharmacologic VTE prophylaxis recommended.
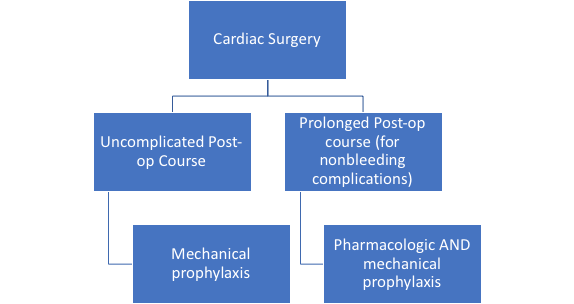
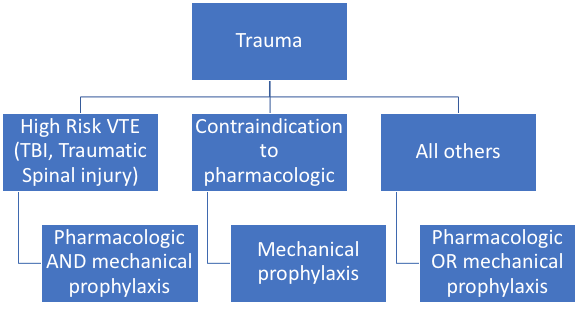
Surgical Patients
- VTE prophylaxis for surgical patients is based on baseline patient risk factors, surgical procedure, and bleeding risk.
- Step 1: Caprini score - estimates patient and surgical risk of VTE.
- Step 2: Estimate bleeding risk - No clear risk stratification model, but grossly estimated based on the following patient factors:
- Bleeding as indication for surgery
- Intracranial hemorrhage
- Moderate or severe coagulopathy, including cirrhosis
- Bleeding diathesis
- Thrombocytopenia
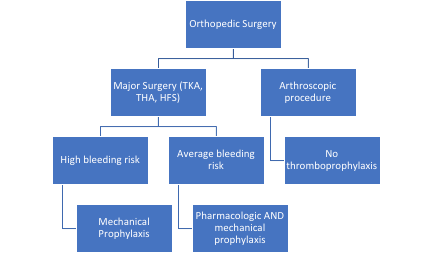
- Step 3: Follow algorithms summarized below
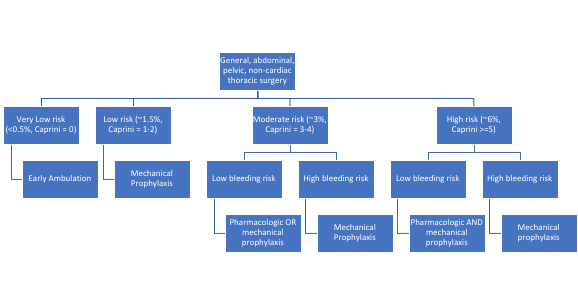

*Patients undergoing surgery for visceral cancer may warrant extended-duration prophylaxis (4 weeks).
Contraindications to Pharmacologic Prophylaxis
- Scoring systems to predict bleeding risk have poor predictive value and have not been well validated in the context of hospital acquired VTE.
- The alternative to pharmacologic prophylaxis is mechanical prophylaxis with intermittent pneumatic compression.
|
Relative Contraindications |
Absolute Contraindications |
|
Mild/Moderate bleeding diathesis Thrombocytopenia (50,000 - 100,000) Coagulopathy Active intracranial lesion (especially vascular lesions) Proliferative retinopathy Vascular access/biopsy sites inaccessible to hemostasis Hypertensive emergency ICH in last 12 months Craniotomy in last 2 weeks GI bleeding in last month |
Active hemorrhage Major bleeding diathesis Active intracranial hemorrhage Thrombocytopenia (< 50,000) Thrombolytics within last 24 hours Spinal or intracranial surgery in last 72 hours Spinal cord injury or TBI with hematoma |
Prophylaxis Regimens:
- LMWH (enoxaparin) 40 mg SQ daily or 30 mg SQ BID
- Unfractionated heparin (UFH) 5000 units SQ BID or TID
- Consider use of UFH instead of LMWH if renal insufficiency (eGFR < 30 mL/min) and/or obesity (BMI ≥40 kg/m2) due to dosing uncertainty. In obesity, consider BID dosing.
- Special considerations
- Orthopedic patients: THA, TKA, HFS require a minimum of 10-14 days post-op course of prophylaxis and often up to 35 days.
- If UFH and LMWH contraindicated (i.e. HIT), discuss with anticoagulation pharmacy to select an alternate agent and see ACCP Guidelines for recommendations.
Geerts, WH, Bergqvist, D, Pineo, GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(6 Suppl):381S.
Guyatt, GH et al. Executive Summary: Antithrombotic Therapy and Prevention of Thrombosis 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2)(Suppl):7S–47S
Kallainen, JS et al. Venous thromboembolism prophylaxis. Institute for Clinical Systems Improvement (ICSI). 2012 Nov. 51 p. http://www.guideline.gov/content.aspx?id=39350
Lim, Wendy. Using low molecular weight heparin in special patient populations. J Thromb Thrombolysis 2010; 29:233–240.
Qaseem, A et al. Venous Thromboembolism Prophylaxis in Hospitalized Patients: A Clinical Practice Guideline from the American College of Physicians. Ann Intern Med. 2011;155:625-632.
Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in Nonorthopedic Surgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST 2012;141(2):e227S-e277S.
Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in Orthopedic Surgery Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST 2012;141(2):e278S-e325S.